肋骨骨折提示存在严重外伤。因此,评估疑似肋骨骨折患者应包括识别骨折及任何并发损伤。并发损伤可高达 90%。[21]Ziegler DW, Agarwal NN. The morbidity and mortality of rib fractures. J Trauma. 1994;37:975-979.http://www.ncbi.nlm.nih.gov/pubmed/7996614?tool=bestpractice.com此外,多发性肋骨骨折的表现还与实体器官损伤概率(约 35%)升高有关。[22]Demirhan R, Onan B, Oz K, et al. Comprehensive analysis of 4205 patients with chest trauma: a 10-year experience. Interact Cardiovasc Thorac Surg. 2009;9:450-453.http://icvts.ctsnetjournals.org/cgi/reprint/9/3/450http://www.ncbi.nlm.nih.gov/pubmed/19541693?tool=bestpractice.com
病史和检查
肋骨骨折最常见于机动车事故 (MVA)、摔倒、遭殴打和工业事故。[1]Sirmali M, Türüt H, Topçu S, et al. A comprehensive analysis of traumatic rib fractures: morbidity, mortality and management. Eur J Cardiothorac Surg. 2003;24:133-138.http://ejcts.oxfordjournals.org/content/24/1/133.longhttp://www.ncbi.nlm.nih.gov/pubmed/12853057?tool=bestpractice.com其他危险因素包括年龄 > 45 岁、骨质疏松症和心肺复苏。患者或急救医务人员可提供重要信息,例如车祸中的钝器伤。驾驶杆的明显侵入表明胸廓遭受了巨大外力。
疼痛和呼吸困难比较常见。胸壁疼痛可损害呼吸动作,导致通气下降。氧合功能受损也可提示潜在的气胸、血胸或肺挫伤。反常的吸气或呼气胸壁运动是连枷胸的体征。多根同侧肋骨发生两处骨折会造成连枷胸,导致胸壁节段不稳定。连枷胸通常伴随其他损伤,且出现威胁生命的气胸、肺挫伤和血胸的风险增加,总体死亡率不低于 5%。[23]Athanassiadi K, Gerazounis M, Theakos N. Management of 150 flail chest injuries: analysis of risk factors affecting outcome. Eur J Cardiothorac Surg. 2004;26:373-376.http://ejcts.oxfordjournals.org/content/26/2/373.longhttp://www.ncbi.nlm.nih.gov/pubmed/15296899?tool=bestpractice.com
需考虑的其他因素:
2% 至 12% 的赛艇选手会因胸腔周期性负荷出现应力性骨折。[15]Smoljanović T, Bojanić I, Troha I, et al. Rib stress fractures in rowers: three case reports and review of literature [in Croatian]. Lijec Vjesn. 2007;129:327-332.http://www.ncbi.nlm.nih.gov/pubmed/18257332?tool=bestpractice.com这也常见于其他越过头顶的重复性体育运动,如棒球和高尔夫球。持续性疼痛和无外伤对诊断具有提示意义。
任何患有已知的恶性病变的人,尤其是肺、前列腺、乳腺、肝脏或胃肠道器官,可能出现癌症肋骨转移。
胸壁原发性骨肿瘤包括骨软骨瘤、内生软骨瘤、浆细胞瘤、软骨肉瘤和骨肉瘤,其自身可表现为肋骨骨折,但比较罕见。其中,恶性病变约占 37%。[8]Aydoğdu K, Findik G, Agackiran Y, et al. Primary tumors of the ribs; experience with 78 patients. Interact Cardiovasc Thorac Surg. 2009;9:251-254.http://icvts.ctsnetjournals.org/cgi/reprint/9/2/251http://www.ncbi.nlm.nih.gov/pubmed/19447801?tool=bestpractice.com多发性骨髓瘤可出现肋骨骨折,甚至是连枷胸。[24]Rammohan G, Karbowitz SR. Spontaneous flail chest in multiple myeloma: successful recovery. N Y State J Med. 1981;81:235-236.http://www.ncbi.nlm.nih.gov/pubmed/6936643?tool=bestpractice.com
若无其他说明,任何儿童或婴儿肋骨骨折均应假设为非意外伤害所致。若无严重外伤,82% 的婴儿和幼儿骨折均是由非意外伤害直接导致。[2]Bulloch B, Schubert CJ, Brophy PD, et al. Cause and clinical characteristics of rib fractures in infants. Pediatrics. 2000;105:e48.http://pediatrics.aappublications.org/content/105/4/e48.fullhttp://www.ncbi.nlm.nih.gov/pubmed/10742369?tool=bestpractice.com在所有骨骼损伤中,身体虐待导致肋骨骨折的可能性最高。[3]Kemp AM, Dunstan F, Harrison S, et al. Patterns of skeletal fractures in child abuse: systematic review. BMJ. 2008;337:a1518.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2563260/?tool=pubmedhttp://www.ncbi.nlm.nih.gov/pubmed/18832412?tool=bestpractice.com
发病率和死亡率
在肋骨骨折病例中,约 14% 至 35% 会发生气胸,约 20% 至 25% 会发生血气胸,约 17% 会发生肺挫伤,约 5.8% 会发生连枷胸;发病率随着骨折数的增加而升高。[1]Sirmali M, Türüt H, Topçu S, et al. A comprehensive analysis of traumatic rib fractures: morbidity, mortality and management. Eur J Cardiothorac Surg. 2003;24:133-138.http://ejcts.oxfordjournals.org/content/24/1/133.longhttp://www.ncbi.nlm.nih.gov/pubmed/12853057?tool=bestpractice.com[13]Keel M, Meier C. Chest injuries - what is new? Curr Opin Crit Care. 2007;13:674-679.http://www.ncbi.nlm.nih.gov/pubmed/17975389?tool=bestpractice.com[14]Liman ST, Kuzucu A, Tastepe AI, et al. Chest injury due to blunt trauma. Eur J Cardiothorac Surg. 2003;23:374-378.http://ejcts.oxfordjournals.org/content/23/3/374.longhttp://www.ncbi.nlm.nih.gov/pubmed/12614809?tool=bestpractice.com
肋骨骨折会损害充分换气功能,导致肺不张、氧合差和呼吸窘迫。第一肋骨外伤性损伤并发大血管损伤的风险为 3%。[16]Gupta A, Jamshidi M, Rubin JR. Traumatic first rib fracture: is angiography necessary? A review of 730 cases. Cardiovasc Surg. 1997;5:48-53.http://www.ncbi.nlm.nih.gov/pubmed/9158123?tool=bestpractice.com
不应忽视老年人的胸壁损伤。老年患者的发病率和死亡率是年轻人的两倍;骨折的肋骨数每增加一根,死亡率增加 19%,肺炎风险增加 27%。[25]Bulger EM, Arneson MA, Mock CN, et al. Rib fractures in the elderly. J Trauma. 2000;48:1040-1047.http://www.ncbi.nlm.nih.gov/pubmed/10866248?tool=bestpractice.com
随着骨折肋骨数的增加,所有年龄组的发病率和死亡率均会明显升高。骨折肋骨数每增加一根,死亡、气胸、肺炎和急性呼吸窘迫综合征 (ARDS) 的风险均会显著增加。6 根肋骨骨折是重症并发症的极限点。[25]Bulger EM, Arneson MA, Mock CN, et al. Rib fractures in the elderly. J Trauma. 2000;48:1040-1047.http://www.ncbi.nlm.nih.gov/pubmed/10866248?tool=bestpractice.com[26]Testerman GM. Adverse outcomes in younger rib fracture patients. South Med J. 2006;99:335-339.http://www.ncbi.nlm.nih.gov/pubmed/16634240?tool=bestpractice.com
检查
初步胸部 X 线检查 (CXR) 是对具有已知的外伤患者的一线影像学检查。[27]American College of Radiology. ACR Appropriateness Criteria: rib fractures. http://www.acr.org/ (last accessed 16 August 2017).https://acsearch.acr.org/docs/69450/Narrative/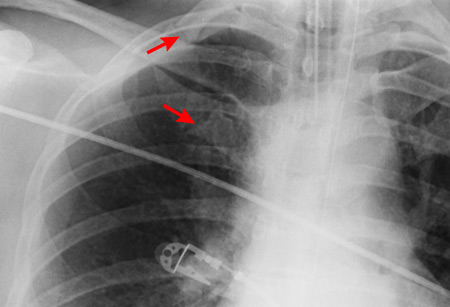 [Figure caption and citation for the preceding image starts]: CXR 显示右侧第一肋骨骨折由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: CXR 显示右侧第一肋骨骨折由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends].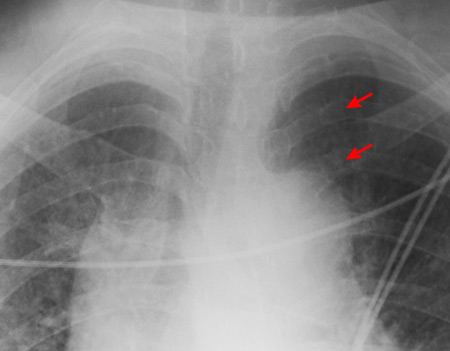 [Figure caption and citation for the preceding image starts]: CXR 显示左后侧多处肋骨骨折由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: CXR 显示左后侧多处肋骨骨折由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends]. [Figure caption and citation for the preceding image starts]: 前后位的 CXR 显示左侧多处肋骨骨折且胸管无移位由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends].,这不仅有助于检测实际肋骨骨折情况,而且还可快速评估气胸、血胸和主动脉损伤情况。然而,常规胸部 X 线对肋骨骨折的漏诊率高达 50%。[28]Livingston DH, Shogan B, John P, et al. CT diagnosis of rib fractures and the prediction of acute respiratory failure. J Trauma. 2008;64:905-911.http://www.ncbi.nlm.nih.gov/pubmed/18404055?tool=bestpractice.com美国放射学会修订了其关于肋骨骨折的适当性标准,建议诊断成人轻微外伤后的肋骨骨折时,无需在胸片基础上再行专门的肋骨放射检查。[27]American College of Radiology. ACR Appropriateness Criteria: rib fractures. http://www.acr.org/ (last accessed 16 August 2017).https://acsearch.acr.org/docs/69450/Narrative/
[Figure caption and citation for the preceding image starts]: 前后位的 CXR 显示左侧多处肋骨骨折且胸管无移位由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends].,这不仅有助于检测实际肋骨骨折情况,而且还可快速评估气胸、血胸和主动脉损伤情况。然而,常规胸部 X 线对肋骨骨折的漏诊率高达 50%。[28]Livingston DH, Shogan B, John P, et al. CT diagnosis of rib fractures and the prediction of acute respiratory failure. J Trauma. 2008;64:905-911.http://www.ncbi.nlm.nih.gov/pubmed/18404055?tool=bestpractice.com美国放射学会修订了其关于肋骨骨折的适当性标准,建议诊断成人轻微外伤后的肋骨骨折时,无需在胸片基础上再行专门的肋骨放射检查。[27]American College of Radiology. ACR Appropriateness Criteria: rib fractures. http://www.acr.org/ (last accessed 16 August 2017).https://acsearch.acr.org/docs/69450/Narrative/
胸部 CT 扫描可提高检测肋骨骨折以及其他损伤的灵敏度。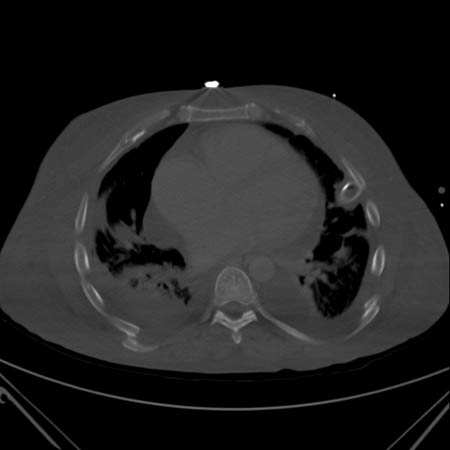 [Figure caption and citation for the preceding image starts]: CT 扫描显示双侧后方肋骨骨折由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: CT 扫描显示双侧后方肋骨骨折由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends].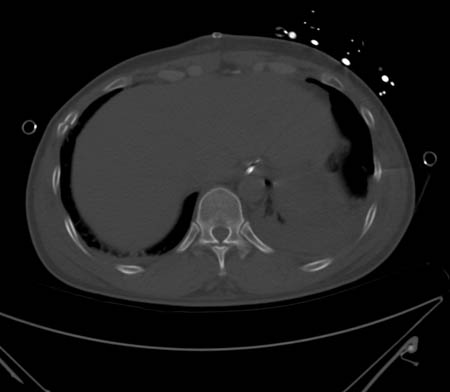 [Figure caption and citation for the preceding image starts]: CT 显示右前外侧肋骨骨折由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: CT 显示右前外侧肋骨骨折由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends]. [Figure caption and citation for the preceding image starts]: CT 显示左后侧节段性肋骨骨折由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: CT 显示左后侧节段性肋骨骨折由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends]. [Figure caption and citation for the preceding image starts]: CT 扫描显示大范围左侧气胸由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends].
[Figure caption and citation for the preceding image starts]: CT 扫描显示大范围左侧气胸由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends]. [Figure caption and citation for the preceding image starts]: CXR 所描绘的气胸与 CT 所示一致由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends]. CT 确实对患者产生严重的放射暴露,但若临床特征提示骨折且确诊后有可能改善患者护理时可考虑使用。美国放射学会修订了其肋骨骨折的适当性标准,声明除在确立进一步护理或作为其他调查(例如虐待老人或法律记录)部分的情形下有必要进行此项评估之外,并无证据表明 CT 检查有益。[27]American College of Radiology. ACR Appropriateness Criteria: rib fractures. http://www.acr.org/ (last accessed 16 August 2017).https://acsearch.acr.org/docs/69450/Narrative/
[Figure caption and citation for the preceding image starts]: CXR 所描绘的气胸与 CT 所示一致由 Paul Novakovich 博士收集提供;经许可后使用 [Citation ends]. CT 确实对患者产生严重的放射暴露,但若临床特征提示骨折且确诊后有可能改善患者护理时可考虑使用。美国放射学会修订了其肋骨骨折的适当性标准,声明除在确立进一步护理或作为其他调查(例如虐待老人或法律记录)部分的情形下有必要进行此项评估之外,并无证据表明 CT 检查有益。[27]American College of Radiology. ACR Appropriateness Criteria: rib fractures. http://www.acr.org/ (last accessed 16 August 2017).https://acsearch.acr.org/docs/69450/Narrative/
近来,超声经评估有助于诊断肋骨骨折。对于诊断肋骨损伤,它的灵敏度是 CXR 的两倍,但其他研究认为超声检查更加费时,也更加疼痛。[29]Bitschnau R, Gehmacher O, Kopf A, et al. Ultrasound diagnosis of rib and sternum fractures [in German]. Ultraschall Med. 1997;18:158-161.http://www.ncbi.nlm.nih.gov/pubmed/9381122?tool=bestpractice.com
血管造影术不是常规检查手段。[16]Gupta A, Jamshidi M, Rubin JR. Traumatic first rib fracture: is angiography necessary? A review of 730 cases. Cardiovasc Surg. 1997;5:48-53.http://www.ncbi.nlm.nih.gov/pubmed/9158123?tool=bestpractice.com然而,可在第一肋骨受损时采用该项检查。
遭受高能冲击后,患者应立即接受胸部和骨盆 X 线检查以排除危及生命的损伤。若患者情况稳定,可在成人中进行头部、颈椎、胸部、腹部和骨盆的 CT 扫描以排除其他损伤。
对于所有疑似遭受身体虐待的儿童,应考虑检查骨骼并咨询儿童保护服务机构。
